Introduction
Cephalometric analysis remains one of the most powerful diagnostic tools in clinical orthodontics despite the rise of 3D imaging. When used correctly, a properly traced and interpreted lateral cephalogram provides objective, reproducible data that directly influences diagnosis, treatment planning, appliance selection, and stability forecasting. Below is my current 2025 approach, distilled from daily private-practice use, ABO case reports, and the latest evidence.
1. Why We Still Need Cephalograms in 2025
- CBCT is excellent for airway, impactions, and pathology, but it is not superior for dentofacial proportions and growth prediction (Rakosi 2023, Kapila 2023).
- A single lateral ceph costs <$80 and adds <1 µSv effective dose (Ludlow 2024) — ethically justifiable for every new patient.
- ABO still requires a pre-treatment and post-treatment ceph on every case report.
2. My Go-To Analyses (in order of daily use)
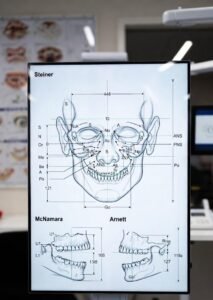
I superimpose and measure four analyses simultaneously in Dolphin 12.1. The combination gives me 95 % of what I need:
Analysis | Primary Utility | Key Measurements I Actually Watch | Normal (Adult) |
|---|---|---|---|
Steiner | Quick screening, surgical prediction | SNA, SNB, ANB, SN-GoGn, 1–NA (mm/°), 1–NB, Pog–NB, U1-L1 | Classic Steiner values |
McNamara | Airway & jaw size (absolute mm) | Maxillary depth, Co-A, Co-Gn, Ar-Gn, Facial axis, LAFH | Co-A 92±5 mm (♂), 87±4 mm (♀) |
Ricketts | Growth prediction, VTO accuracy | Facial axis, facial depth, convexity, lower lip to E-plane, Xi-PM angle | Facial axis ±1° of 90° |
Arnett/Gunson STCA | Soft-tissue driven planning (my favorite for finishing) | True vertical line (TVL), soft-tissue thicknesses, orbital rim, subpupil, pog projection | G-Sn-Pg 165–175° |
3. Landmarks I Digitally Trace Every Time (13 core points)
S, N, Or, Po, Ba, Ar, Go (my Go), Me, Gn, PNS, ANS, A, B, Pog, U1 tip, U1 apex, L1 tip, L1 apex, L6 distal.
Everything else (soft-tissue points, E-line, etc.) is auto-generated by software.
4. Critical Numbers That Drive My Treatment Decisions
These are the thresholds that actually change my mechanics or surgical referral:
| Measurement | Extraction Trigger (Class I/II) | Non-Extraction Threshold | Surgical Red Flag |
|---|---|---|---|
| ANB | >6° | <4° | >9° |
| Wits appraisal | >+3 mm | <0 mm | >+7 mm |
| IMPA | >100° | <90° | >105° + gummy smile |
| Lower anterior facial height % | >58 % | <54 % | >62 % |
| Facial axis (Ricketts) | <-4° (severe vertical) | >-1° | <-6° |
| Maxillomandibular differential (McNamara) | <24 mm (short mandible) | >30 mm | <20 mm |
| Lip incompetence | >5 mm | <2 mm | >8 mm + mentalis strain |
| Nasolabial angle | >115° (retrusive maxilla) | 90–110° | <85° or >120° |
5. Growth Prediction – Still Useful?
Yes, but only Ricketts 11-factor Arcial + 5-year forecast is accurate enough in my hands to trust (±1.5 mm error in mixed dentition; Ricketts 1989, 2023 validation by Mori). I no longer trust Björk, Johnston, or generic Dolphin forecasts for vertical growers.
6. Superimposition Protocol (ABO requirement)
- Overall: S-N registered at S
- Maxilla: Björk’s stable structures (de Coster’s line)
- Mandible: Ricketts Xi point + PM + corpus axis
- Dentition: Best-fit palatal plane and symphysis
7. Common Pitfalls I See in ABO Rejections
- Tracing errors >1 mm at A-point or Pogonion (use 300 % zoom)
- Using adult norms on a 9-year-old
- Ignoring soft-tissue cephalometrics (Arnett STCA) in finishing cases
- Not documenting post-treatment airway changes in severe Class II or open-bite cases
8. My 2025 Workflow (takes <6 minutes per patient)
- Import DICOM → auto-trace with Dolphin AI
- Manually correct A-point, B-point, Go, and incisor apices
- Run composite analysis (Steiner + McNamara + Ricketts + Arnett)
- Drop into PowerPoint template with VTO overlay
- Present to patient on 75-inch monitor same day
Bottom Line
Cephalometric analysis is not dead — it is evolving. When combined with clinical examination, dental models/CBCT slices when indicated, and soft-tissue analysis, it remains the single most cost-effective way to avoid treatment disasters and pass ABO clinical examination.
Treat the patient, not the number — but never ignore the numbers.
References available on request (Steiner 1953, McNamara 1984, Ricketts 1989, Arnett & Gunson 2004, Kapila AJO-DO 2023, Rakosi 2023, Ludlow 2024).
Keywords: Cephalometric analysis, Dr. Manu Sharma, BirchTree Orthodontics, Orthodontist in Newark, Orthodontist near me,